Why the painful spot is rarely the cause
Patients point to where it hurts, and conventional care often follows the finger: image the lumbar disc, name the herniation, treat the site of the symptom. Yet experienced manual therapists keep meeting pain that refuses to resolve when only the painful region is addressed. Fujii’s starting premise is blunt — the place that hurts is frequently not where the problem lives.
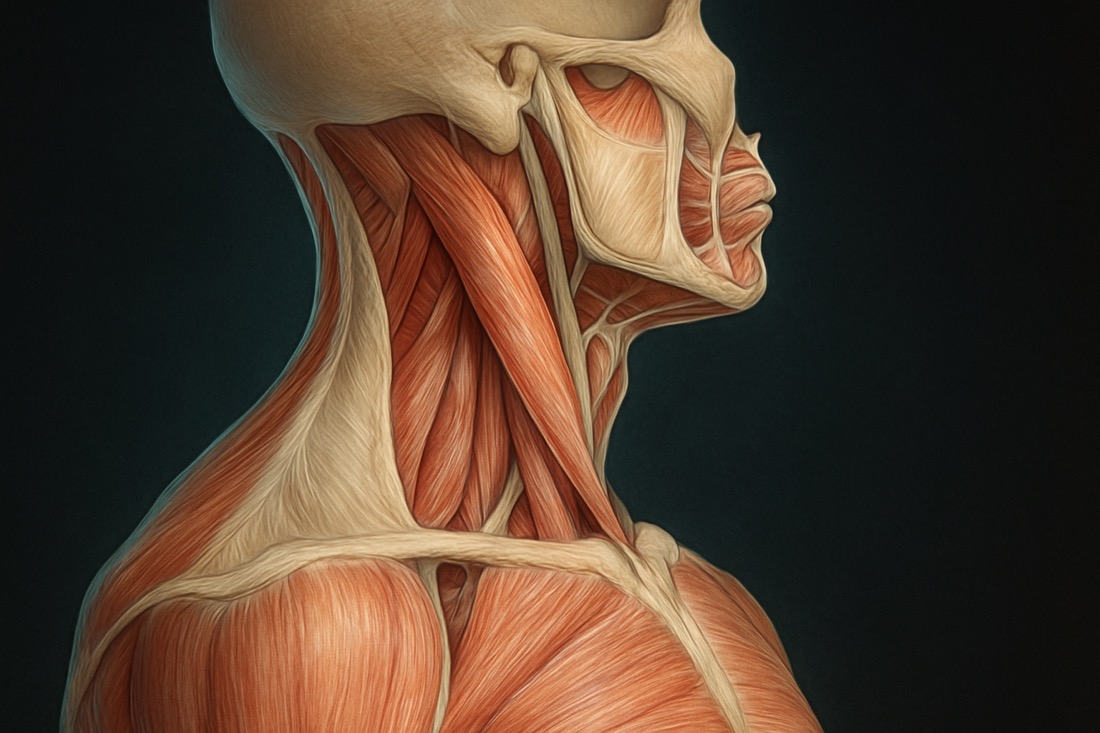
Connective tissue offers a mechanism for this everyday observation. Fascia forms a continuous, body-wide network that mechanically and chemically links distant regions, behaving less like isolated parts and more like a single responsive fabric [1]. When that fabric is loaded, densified, or restricted in one area, symptoms can surface somewhere else entirely. Treating only the loud, painful site leaves the quiet driver untouched — which is exactly why so many interventions produce partial, short-lived results.

Read the body as a map: the fascial chains
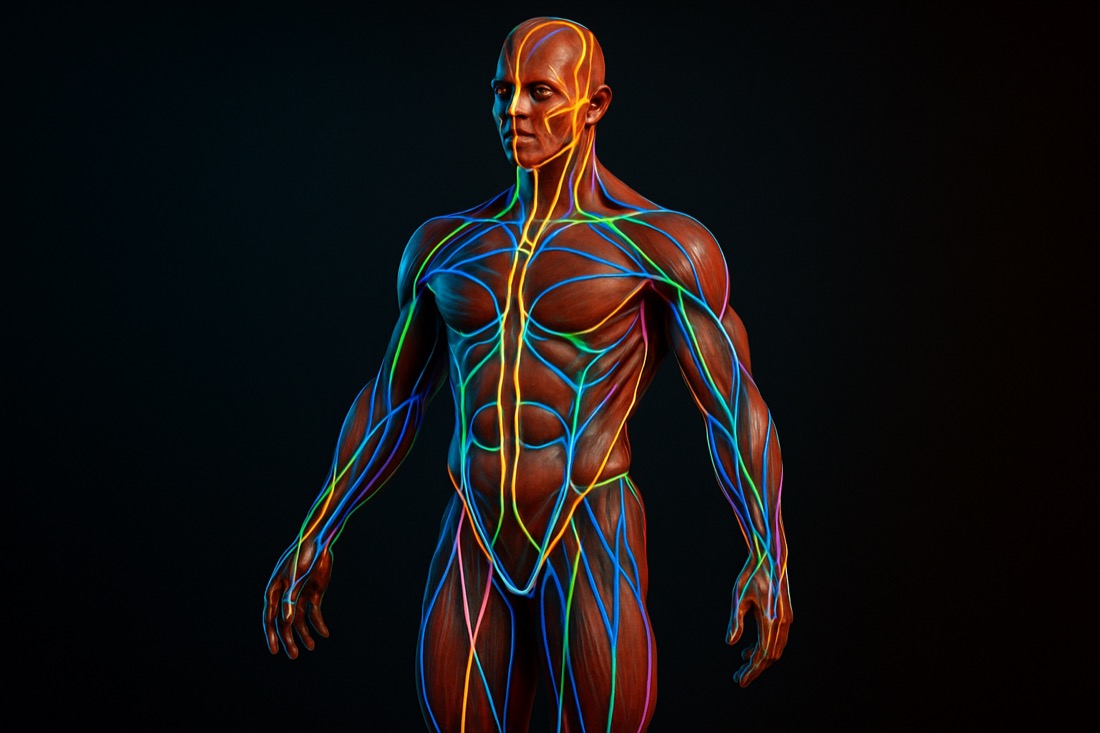
Before touching anything, Fujii reads the body as a connected system. Tension travels along recognizable myofascial routes — the “anatomy lines” — so a complaint at the low back may trace to the hips, the posterior chain, or the neck. Knowing this map is what lets a clinician look past the symptom and ask where the line is actually being pulled.
The evidence here is appropriately cautious but real. Systematic reviews find moderate anatomical support for several myofascial continuities, and cadaveric studies confirm that force can be transmitted along these chains rather than staying neatly within a single muscle [2][3]. For the practitioner, the takeaway is practical: assessment should follow the connections, not the borders drawn in an anatomy textbook.

Assessment first: finding the pain generator
The decisive skill, in Fujii’s words, is assessment — and it is where most treatment goes wrong. He calls the target the pain generator (発痛源): the specific tissue actually driving the complaint. Misidentify it and every subsequent technique, however skilled, is wasted effort applied to the wrong place. The clinicians who get reliable results are simply faster and more accurate at locating that source.
Assessment is not guesswork. By applying light, graded mechanical input and reading how the tissue and the symptom respond, the therapist narrows in on the generator and predicts how it should change. This “test, treat, re-test” discipline turns a hopeful technique into a measurable hypothesis — and it is the part of the craft that beginners most often skip.

Light mechanical input: how fascia responds
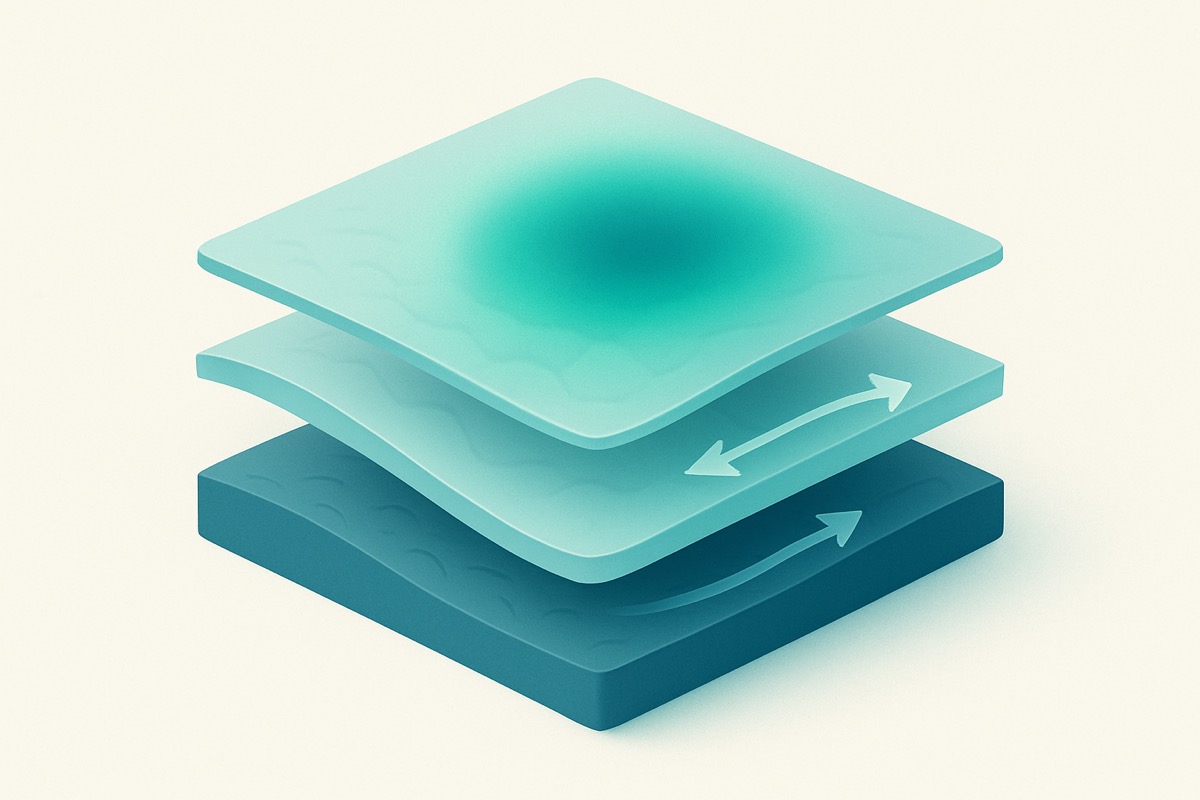
Once the source is mapped, the input is often gentler than expected. Densified fascia is not simply “tight muscle” to be forced; it is connective tissue whose behavior changes with hydration, glide, and load. Light pressure and graded stimulus can shift the local environment — including the hyaluronan-rich layers between fascial planes that, when altered, are implicated in myofascial pain [4].
This is why heavy, painful pressure is rarely the answer. The goal is to restore normal sliding between layers and to give the nervous system new, non-threatening information, not to overpower tissue. Quality of contact and direction matter more than force.
The release: restoring glide and calming the system
Release is the visible part of the work — but Fujii frames it around a sensation: what it feels like when the body actually lets go of pain and numbness. Controlled trials of myofascial release report meaningful improvements in pain and function for non-specific neck and low-back complaints, even if the literature is still maturing [5][6].
Part of the effect is mechanical and part is neurological. Fascia is richly innervated, and hands-on input appears to modulate tone and the autonomic state, not just stretch collagen [7]. That dual action helps explain why a precise, well-targeted release can produce a change a patient feels immediately.
What “instant relief” really means — and its limits
Immediate change is real and increasingly measurable: tools such as ultrasound elastography can quantify shifts in tissue stiffness before and after manual therapy, moving “it feels better” toward something objective. A single session can genuinely reset a pattern when the generator is found and addressed.
It is not, however, a cure-all. Durable results depend on load management, movement, and the patient’s broader health — and dramatic on-camera demonstrations are teaching tools, not guarantees. This article is educational and intended to support qualified clinical practice; it is not medical advice, and persistent or severe symptoms should be evaluated by a licensed professional.